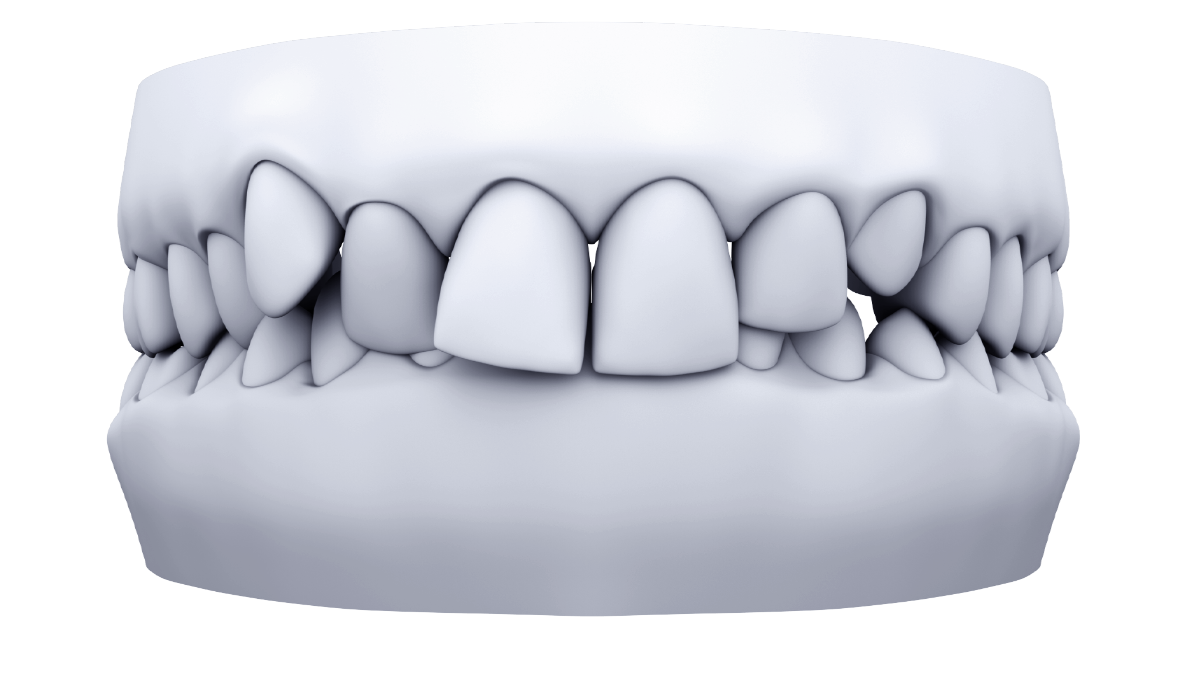
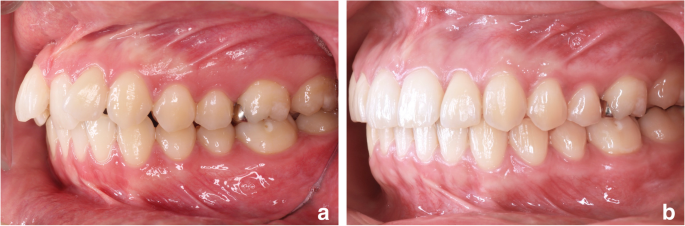
Deep bite
This type of malocclusion can cause:
- excessive attrition of the anterior teeth over time;
- super eruption of anterior teeth;
- lingual inclination of anterior or posterior teeth. Uprighting posterior teeth will open the VDO and can provide 2-3 mm of bite opening in the anterior segment
There are 4 possible components for deep bite correction. Not all these components apply to
every case.
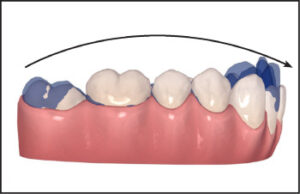
- Leveling the Curve of Spee which often involves anterior intrusion and in some
cases extrusion of premolar teeth. - Leveling the Curve of Wilson which is uprighting lingually tipped posterior teeth.
- Posterior aligner Anchorage to prevent slippage during anterior intrusion.
- Proclination of Retroclined Anterior Teeth.
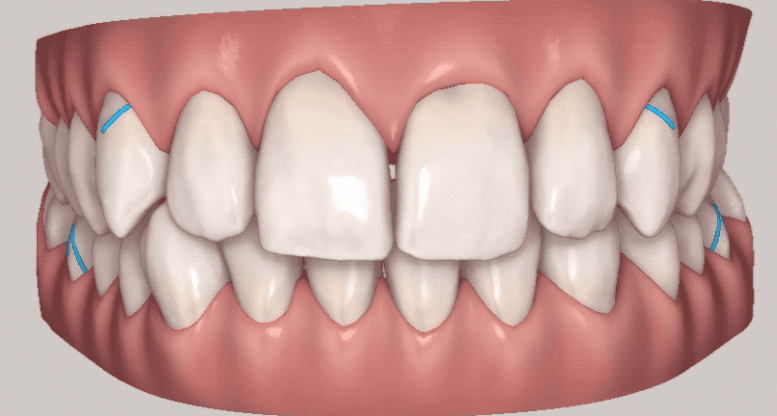
Deep bite attachments
Add Horizontal-Incisal-Beveled attachments to available posterior teeth in extremely deep
bite cases. Goal = 1 per quadrant. This will boost anchorage. Only add on teeth without
attachments. Avoid 2nd molars.
Request attachments that HBAs are 4 mm wide and 1.25 mm thick, angulated gingivally.
Posterior and mandibular anterior attachments should be moved as incisal or coronal as possible where the aligner force levels are strongest, without interfering with occlusion.
Attachments are often unnecessary for teeth undergoing intrusion, with the exception of the mandibular canines if more than 1 mm mandibular incisor intrusion is needed (horizontal beveled attachments.)
Elastics for deep bite correction
Elastics assist in mandibular molar extrusion (when programmed into the virtual treatment plan) and mandibular incisor proclination; therefore, they can be utilized even for Class I patients.
| Triangular elastics (for Class II correction + extrusion/to level Curve of Spee) |  |
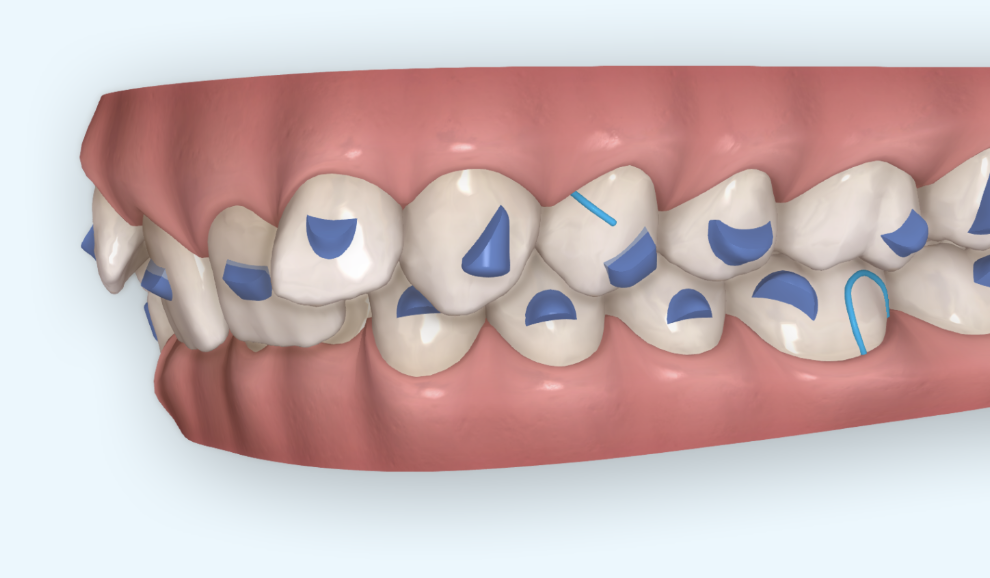
Occlusal Contacts
- Strong contacts from 7th to 4th (red) and LIGHT from canine to canine (or no contact)
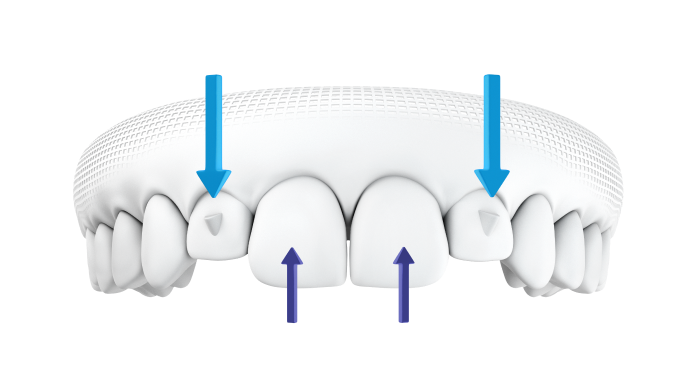
Overtreatment of overbite
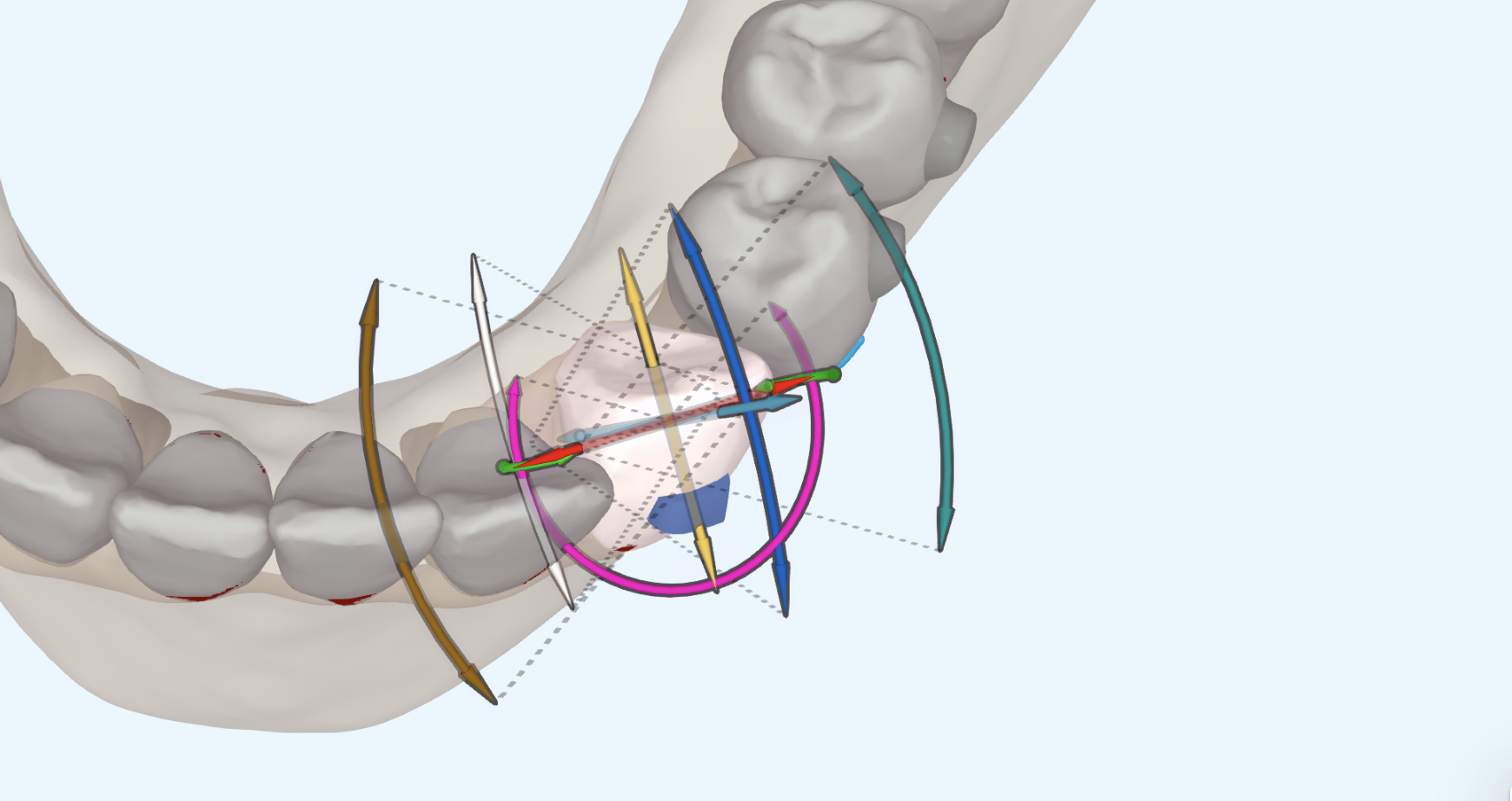
In extreme deep bite cases add additional anterior intrusion. Set overbite at 0-1mm. Use the 3D Controls and set the upper incisal plane first. Then, add additional lower anterior intrusion.
Overtreatment of overjet
Create 1-2mm of excess overjet in deep bite cases.
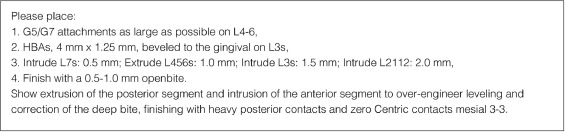
Prescription for leveling deep curve of Spee:
“Intrude mandibular second molars 0.5 mm, extrude premolars and first molars 1.0 mm, intrude canines 1.5 mm, and intrude incisors 2.0 mm. Finish with a 0.5 – 1 mm open bite with heavy posterior contacts”
If the curve of Wilson is steep (posterior teeth are lingually inclined):
Prescribe 5° of buccal crown tip to the mandibular premolars and molars.
Clincheck instruction requesting temporary spacing to facilitate anterior rotation, extrusion, and intrusion:
“Please move _____ teeth forward to create temporary interproximal spacing. Do NOT perform any rotation, intrusion, or extrusion until this space has been created. Then perform the necessary movements. Maintain this space until all these movements are completed. Use hinge axis mechanics for all rotations. Once all these movements are complete retract lingual to close all interproximal spacing.” (Hint: Use this instruction if there are anterior extrusions, intrusions, and/or rotations)
Clincheck instruction requesting additional intrusion when you want to over-treat the deep bite:
“The current Clincheck includes anterior intrusion as a result of leveling. I like to “over-treat” intrusion. Please perform additional intrusion so that there is .5mm of overbite with the central incisor teeth. Intrude upper ____ (specify teeth) ___mm and the remainder with the L3-3 teeth. All intrusion stages are to be included in regular (NOT over-correction) stages.” (Hint: decide if any upper incisor intrusion is needed for aesthetics and specify the amount. Example: 2 mm of intrusion for 8-9)
Clincheck instruction requesting bite ramps:
Please add precision bite ramps for teeth 7-10. If the anterior bite does not allow ramps on all these teeth go ahead and add them to the teeth allowed. If no ramps can be placed substitute with cuspid ramps. Once the bite will allow precision ramps remove the cuspid ramps and replace them with the precision ramps.”














{kind=link}