Troubleshooting. Posterior open bite etiology and solutions
What may lead to a posterior open bite with aligners?
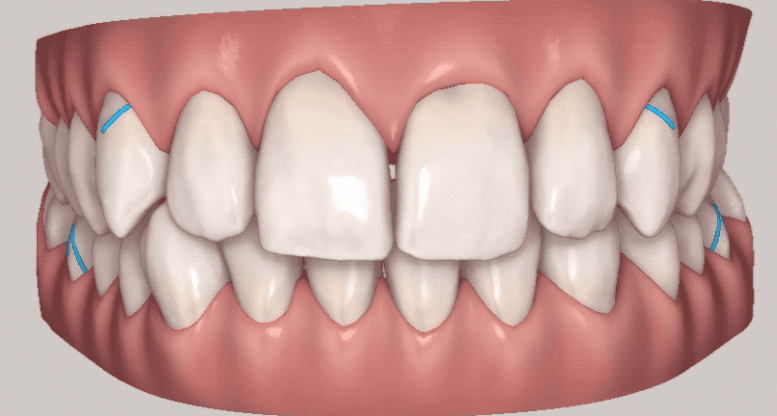
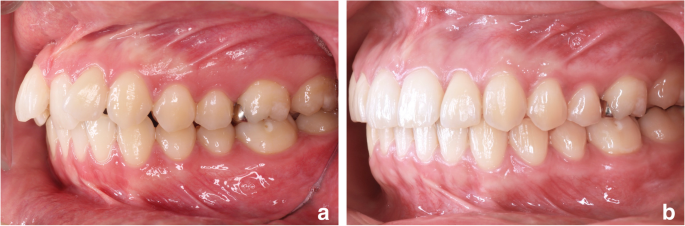
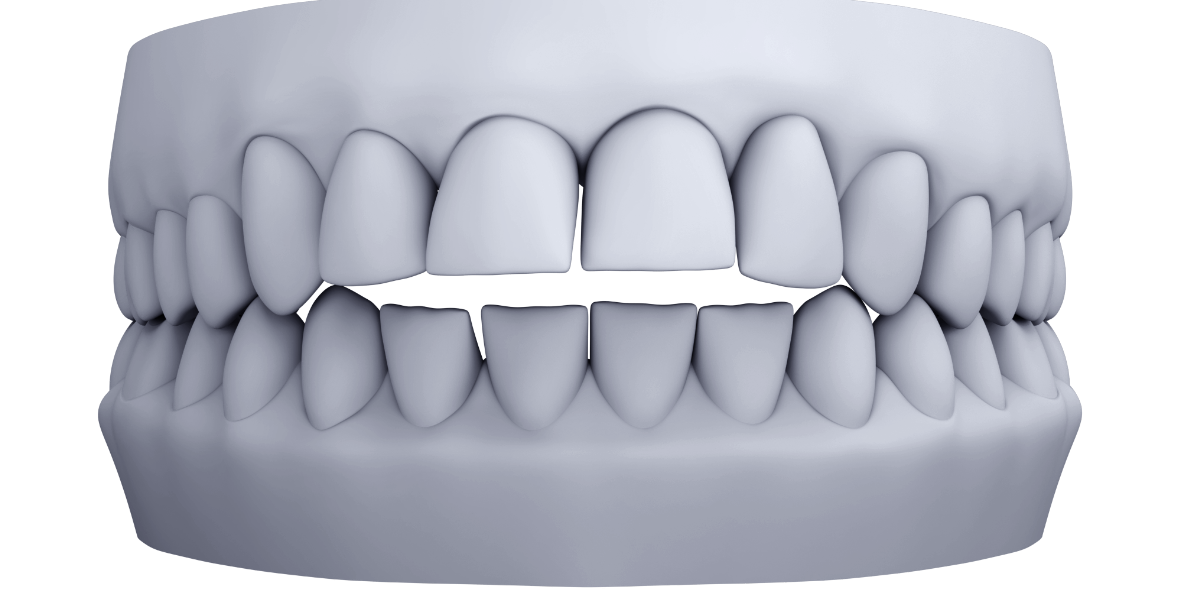
- Lack of overjet/heavy anterior centric contacts:
- undiagnosed TSD (tooth size discrepancy)
- insufficient bite opening – and lack of anchorage to intrude
- Insufficient anterior torque
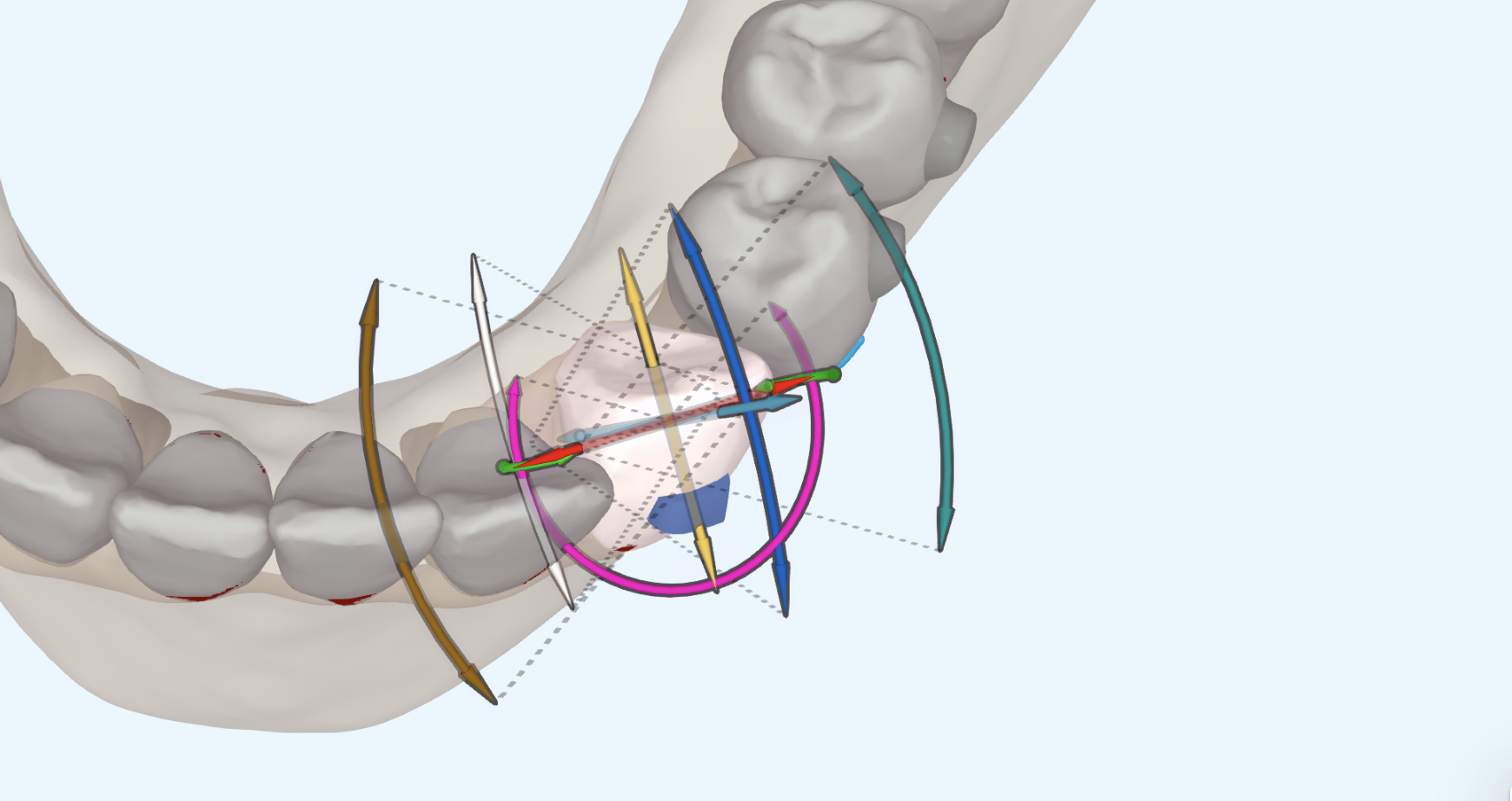
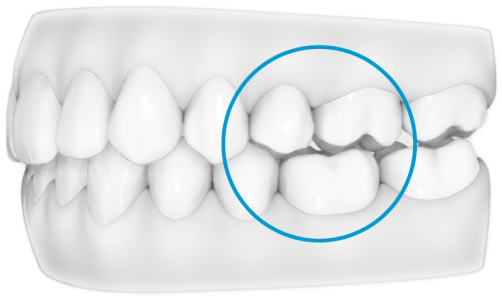
2. Transverse correction when axial inclinations are already upright/ in buccal-version. It is important to note the Curve of Wilson, especially if any maxillary expansion has been produced. Often the palatal cusps of the molars and perhaps premolars may be more prominent (or “hanging”), causing the appearance of an open bite.
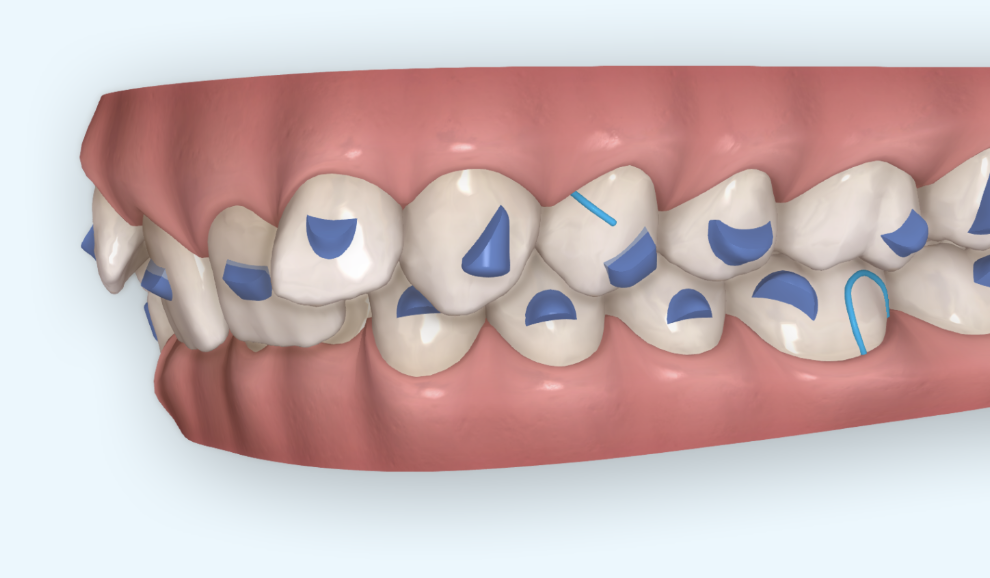
3. Lack of proper movement expressed with the aligner (i.e. roatations)
4. Lack of anchorage considerations with a bite jump (i.e. autorotations)
5. Patients who are clenchers/active posterior intrusion
6. Lack of molar attachments when mesial, distal or extrusive movement is noted
7. Unanticipated growth – i.e. all class I teenagers should have Class III elastics
8. Mandibular distalisation attempts
9. Inaccurate bite set
10. Improper bite closure mechanics
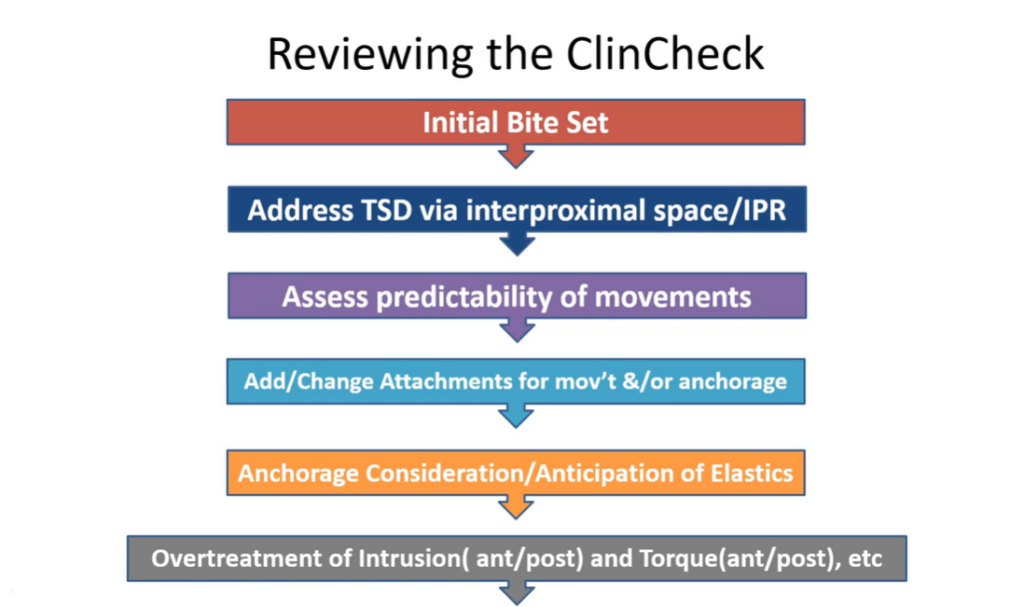
Review Chlincheck
Solutions:

- Adding buccal root torque for posterior teeth during treatment may reduce prominent palatal cusps of molars.
- Adding some mild intrusion for second molars may also be necessary to close mid arch openbites.
- Aligners can be sectioned distal to cuspids to allow for some settling as well as to close posterior open bites.
- Use of “seating” intermaxillary elastics
Key Points
- If the posterior open contacts are 1 mm or less, consider allowing time for natural settling combined with equilibration.
- In bilateral POB cases, you can cut the aligners distal to the cuspid teeth. Allow about 4 to 6 weeks of settling, consider equilibration, and then take records to finish the case.
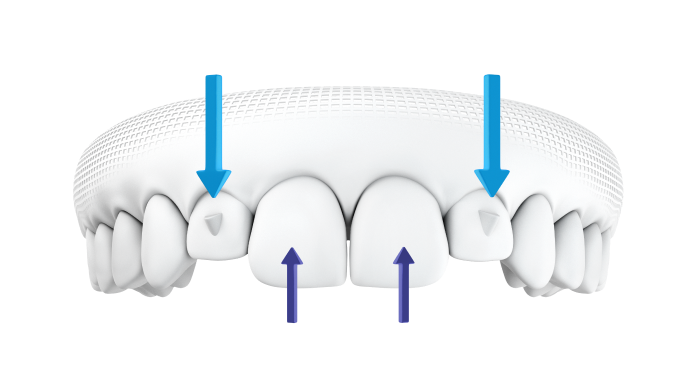
- If there are premature anterior contacts, request additional aligners with an anterior open bite. Over program the anterior open bite into the Clincheck. Request a bite closure simulation showing the effect of removing the premature anterior contacts.
Clincheck instruction to correct a posterior open bite where the cause is a heavy anterior occlusion:
“There are premature occlusal contacts associated with teeth ______. These are contributing to a posterior open bite. Create 2mm of bite relief for these teeth. Perform all or any of these movements to create the relief: anterior intrusion, anterior torque, and lower anterior lingual retraction to create overjet. I want to see 2mm of open occlusal contacts for these teeth. Then at the last regular stage create an occlusal jump simulating auto rotation of the mandible into a fully closed position. Do NOT treat the posterior open bite with posterior extrusions. Treat it with anterior bite relief.”